
How to Write a Nursing Care Plan: With Examples

Nursing students learn to evaluate a patient, make a diagnosis, formulate, implement, and create a care plan to provide individualized care and guarantee the best healthcare outcomes. By developing a well-designed care plan, nursing scholars can ensure the delivery of personalized, evidence-based, and patient-centered care through systematic organization. Are you a DNP student searching for a nursing care plan writing service? This is where your search ends. Our company has experienced specialists with proven backgrounds, field expertise and nursing degrees, helping nursing scholars develop the various types of nursing papers, such as essays, dissertations, SOAP notes, and capstone projects, among others.
Our company has a skilled team of writers who help scholars compose nursing care plans that address specified requirements. Hire an expert to write a nursing care plan from our company and enjoy professional DNP-level writing services, round-the-clock consultancy, timely delivery without compromising on quality, and free revisions. In this article, we have highlighted the 5 main components of a nursing care plan and various examples of nursing care plans for hypertension and pneumonia.
What is a Nursing Care Plan?
The nursing care plan is a personalized and comprehensive strategy that is used to identify a patient’s potential needs or risks to help nurses achieve positive healthcare outcomes. The nursing care plan consists of the patient’s goals, the nurse’s diagnosis, interventions required to achieve the identified goals, and an assessment of the patient’s response to the said interventions. In case you need help writing nursing care plans and other nursing papers, such as SOAP notes, DNP projects, nursing research papers, and DNP data analysis, reach out to us now to have your paper customized as per your requirements by the best nursing writers.
Formulating an excellent nursing care plan supports nurses in their ability to:
- Demonstrate the patient’s past and present medical status and current needs to all healthcare practitioners involved in providing care.
- Communicate information about successful approaches and patterns of patient responses to certain interventions.
- Ensure the continuity of care when a patient leaves a hospital setting while still needing medical services.
- Critically think about the needs of each patient and develop a tailored plan.
- Outline assessments to be made, healthcare issues to be addressed, nursing actions to conduct, and outcomes to evaluate.
- Communicate among other members of the medical team about the patient’s condition, needs, and interventions, thereby facilitating an integrated and efficient care delivery.
What are the 5 Components of the Nursing Care Plan?
1. Assessment
The assessment involves the systematic collection and analysis of client data. Conducting the assessment is crucial as it serves as the foundation for the development of the nursing care plan and as the guidelines for measuring the plan’s effectiveness. In the assessment section, the registered nurse applies their critical thinking, perceptual, and observational skills to collect subjective and objective data directly from the patient or caregivers. Subjective data is verbal statements from the patient, and objective data is measurable data such as height, weight, vital signs, lab results, and observable patient behaviors.
2. Diagnosis
The diagnosis is the nurse’s clinical judgement about the patient’s response to the actual or potential medical conditions on the part of the patient, family, or community. The diagnosis section illustrates not only the pain of the patient but also the issues the ailment has caused, such as imbalanced nutrition, depression, anxiety, or family conflict, among others. A well-formulated nursing diagnosis should be based on the North American Nursing Diagnosis Association (NANDA) diagnosis list guidelines and aligned with Maslow’s Hierarchy of Needs to ensure that it is patient-centered. Maslow’s Hierarchy of Needs is applied in the diagnosis section of the nursing care plan to ensure that important physiological, safety, and security needs are met before addressing other needs such as self-actualization and esteem. Formulating a nursing diagnosis by applying the NANDA diagnosis list and Maslow’s Hierarchy of Needs helps in the planning and implementation of effective patient care.
3. Planning
The planning stage involves formulating a strategy that prescribes methods and alternatives that can be employed to achieve the expected outcomes. Based on the data collected during assessment and diagnosis, the nurse sets achievable short and long-term goals that directly impact patient care and are based on evidence-based practice guidelines. The specified actions and interventions are selected to assist the patient in achieving the desired state of outcomes and discharge goals. The set goals should be: (i) Specific, (ii) measurable, (iii) attainable, (iv) realistic, (v) time-oriented.
4. Implementation
Implementation is the step that involves carrying out the nursing interventions stated in the nursing care plan. The nursing interventions should be clearly stated and specific, starting with an action verb illustrating what the nurse is supposed to do. The registered nurse should also use qualifiers such as how, when, and where to provide the content about the planned activity. In the implementation section of the nursing care plan, the nurse should specify interventions such as direct or indirect care, medication administration, applying a cardiac monitor, or standard treatment protocols.
5. Evaluation
Evaluation encompasses collecting data and comparing it with desired outcomes, analyzing the patient’s response, identifying factors that enabled the success or failure of the care plan, adjusting the plan, and planning for future nursing care. When writing the evaluation, the nurse uses subjective and objective information from the patient to assess their progress. Based on the results, the nurse determines whether the interventions are effective in meeting the patients’ needs, and if there is a positive advancement, the care plan may continue. However, if the patient’s needs are not being met, modification to the care plan is made.
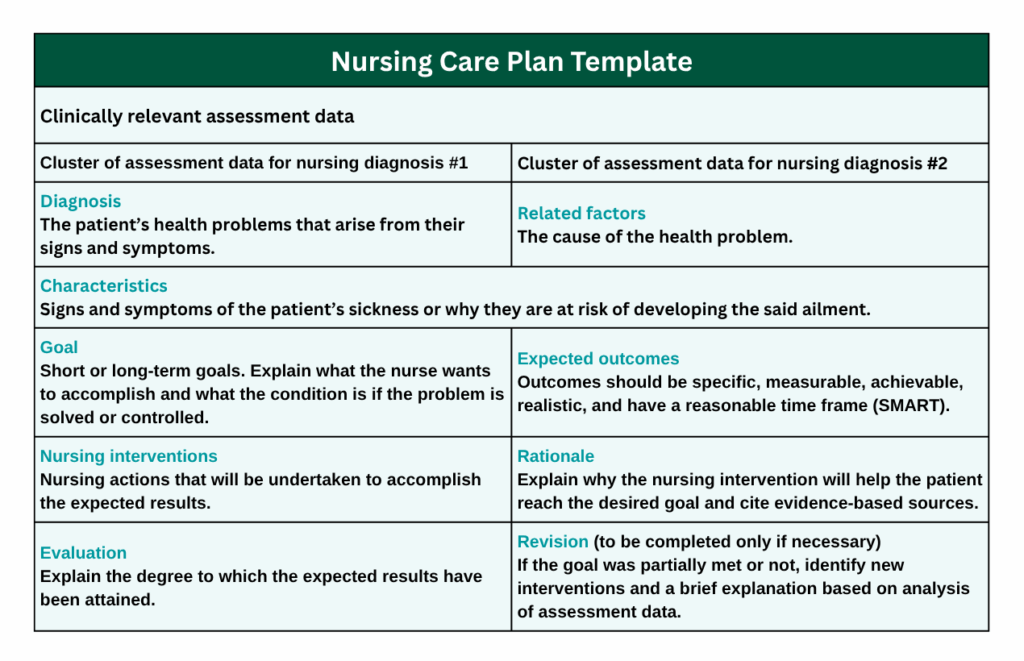
Nursing Care Plan Template
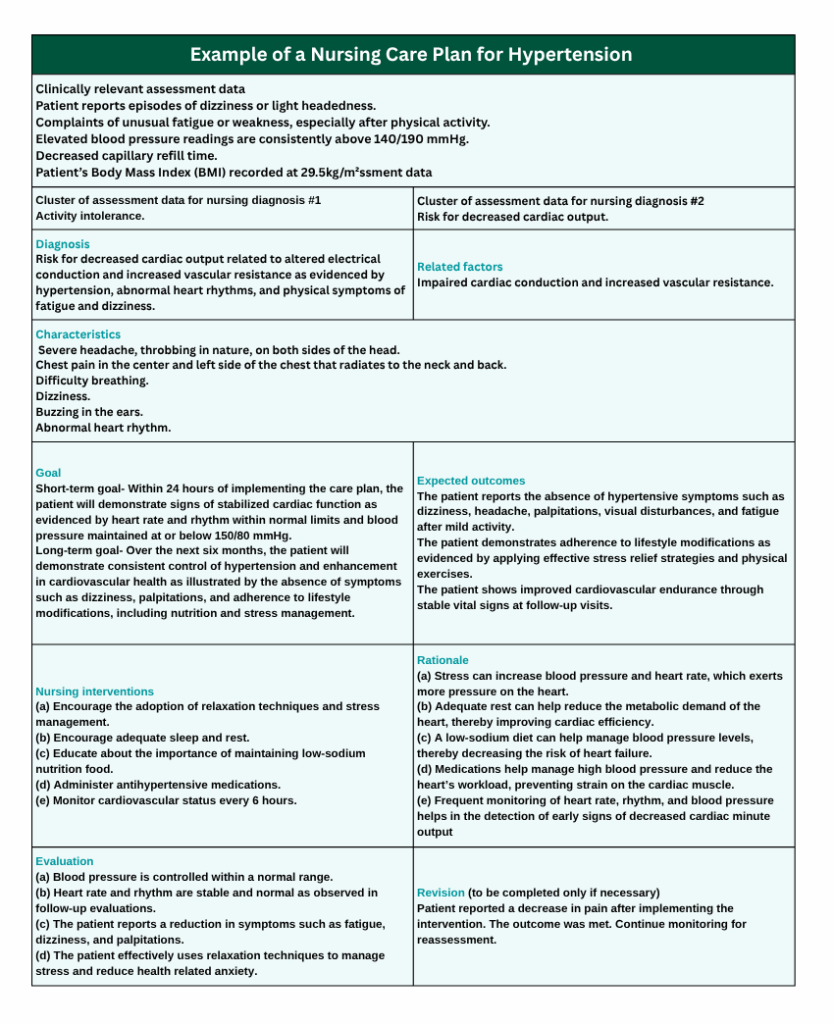
Example of a Nursing Care Plan for Hypertension
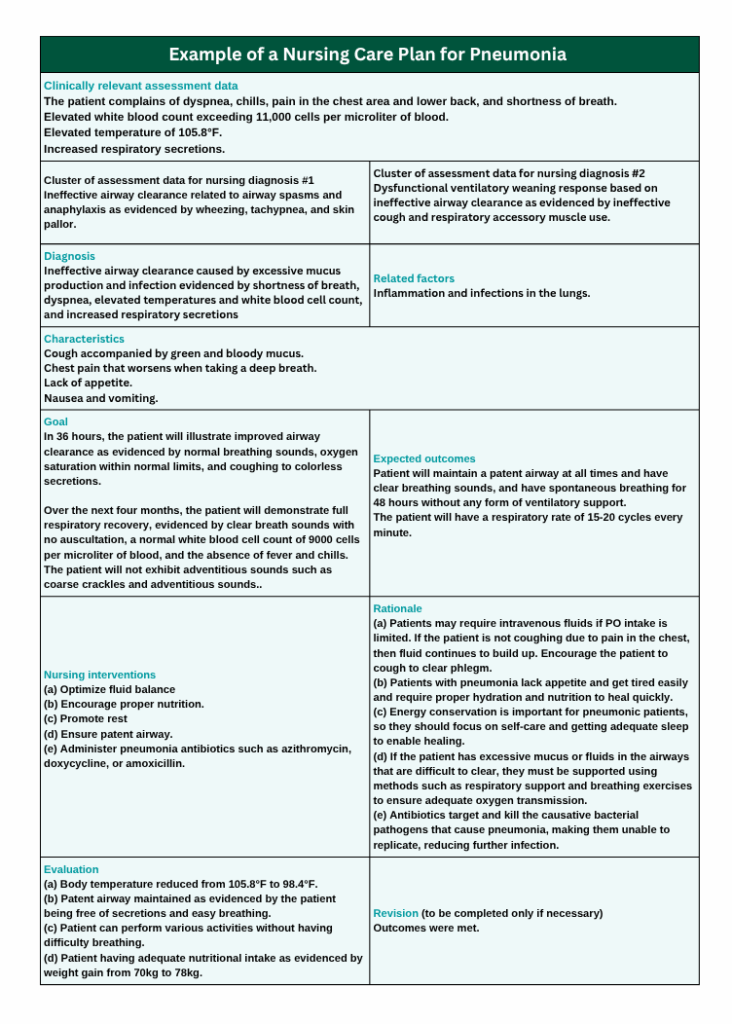
Example of a Nursing Care Plan for Pneumonia
Summary
A nursing care plan is a personalized and comprehensive strategy that is used to guide nursing care and achieve patient-centered healthcare outcomes. The nursing care plan comprises an assessment, diagnosis, planning, implementation to meet goals, and evaluation of the client’s response to the interventions. Nursing care plans are used to structure interventions and personalize them to patient goals, thereby providing standardized care across various healthcare environments from admission to discharge.
Might you be looking for expert help on nursing care plan writing? Let our certified DNP-level experts compose original, quality nursing care plans for you. We deliver original human-written nursing care plans on time, without compromising on quality. Additionally, we offer free revisions until our clients are satisfied with the work, and that’s why most nursing students and professionals trust us with their tasks. We write other nursing papers, including discussion posts, reflection papers, systematic reviews, DNP projects, and PowerPoint presentations, among others. To enlist our nursing care plan writing services, contact our professional consultants now to get started. We are available 24/7 to serve our clients at their convenience. Contact us now, or talk to our friendly customer service agent via our live chat. It doesn’t matter to us how complex the case is and how short the urgency is; our excellent writers handle your nursing care plan with ease and deliver the best paper, right on time.